

FAMILY PLANNING, a term for programs to regulate family size that came into use in the West in the 1930s. Although it originally encompassed efforts both to promote and to curtail fertility, explosive population growth in the developing countries since mid-century has narrowed its meaning to control of fertility, including programs for prevention of conception, abortion, and sterilization.
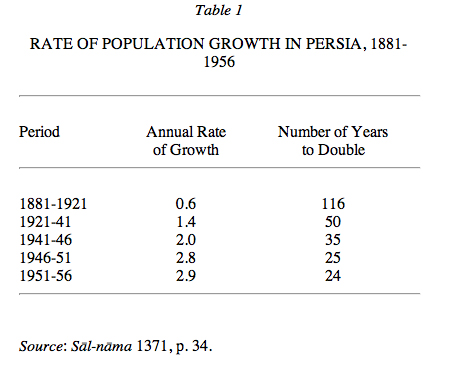
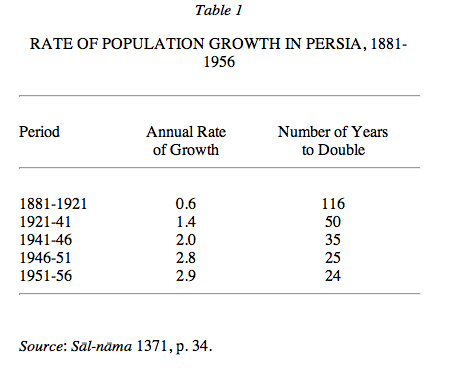
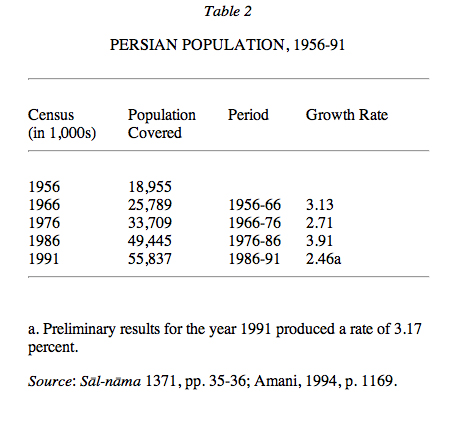
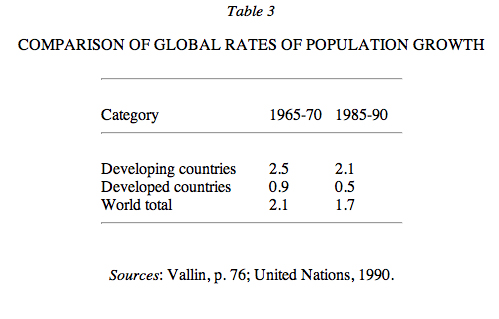
Government-sponsored family-planning programs were introduced in Persia in the 1960s in response to accelerating population growth since the turn of the 20th century, among the highest in the world (Table 1; Table 2; Table 3). In 1981-83 Persia ranked twenty-first in the world in population and fifteenth in population in the age group fourteen years old and under, but a decade later it ranked sixteenth and thirteenth respectively (Table 4). It is predicted that it will rise to eleventh in total population by the year 2025 (Bulletin, 1991, p. 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
EARLY EFFORTS
In Persia interest in demographic growth within the framework of economic development manifested itself rather timidly in the first and second national economic plans (1948-56, 1956-61). In the third (1962-68) more importance was allotted to curbing population growth. Before family planning was officially adopted, however, the government and some private agencies had already taken measures to encourage birth control. For example, the Association for the Protection of Mothers and Children (Anjoman-e ḥemāyat-e mādarān o kūdakān), a private institution established in Tehran in 1954 under the direction of Moḥammad Moʾtamanī, provided limited assistance with contraception. The following year a government department dealing with maternal and neonatal health was established in the Ministry of Health (Wezārat-e behdārī); it dispensed advice, mostly in Tehran, on birth control and, to a limited extent, provided contraceptive devices. In 1957 the Association for Family Orientation and Assistance (Anjoman-e rāhnemā-ye ḵānavāda), another private institution, was founded in Tehran, with the help of the London-based International Planned Parenthood Federation. Its first director was Sattāra Farmānfarmāʾīān, dean of the Tehran School of Social Work, and its purpose was to provide both advice on family planning and birth-control devices, particularly foam-tablet spermicides and condoms. In 1964 a number of religious leaders, including Ayatollah Shaikh Bahāʾ-al-Dīn Maḥallātī, approved family planning, provided that it be a short-term solution (i.e., a reversible method) and not permanent (Dānešgāh, pp. 32-41).
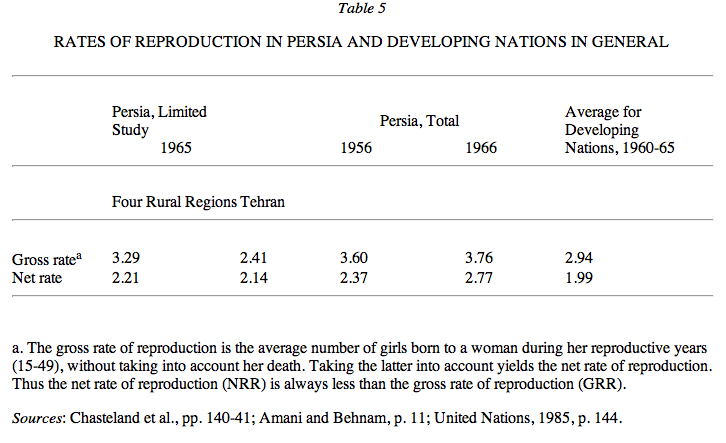
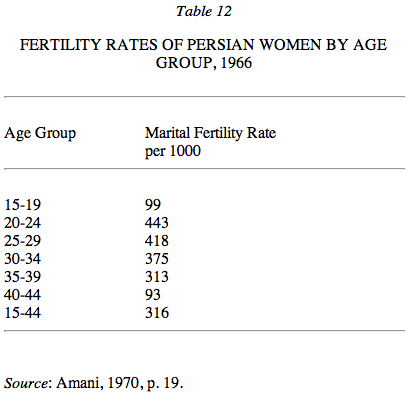
The demographic section of the Institute for Social Research at Tehran University, with United Nations technical cooperation, conducted two studies on fertility in four rural regions and Tehran in 1965. In both gross and net rates of reproduction Persia surpassed other developing countries (Chasteland et al., pp. 140-41; (Table 5). The total fertility rate, that is, the total number of births, both male and female, for a woman during her period of fertility, was an estimated 7.98 and 8.4 for women married at the ages of twenty and fifteen years respectively in 1956, though even ten years later 2.7 would have been necessary to ensure zero population growth. Meanwhile, according to United Nations figures (1985, p. 398), the Persian mortality rate was declining (Table 6).
{kind=link}
{kind=link}
The results of the 1966 census (q.v.) pressed home the dimensions of the problem, an annual population-growth rate of 3.13 percent for the preceding decade, higher than the average of 2.3 percent for all developing countries. In that year a committee of representatives from several government ministries, Tehran University, and private institutions was established within the Plan Organization (Sāzmān-e barnāma) to develop a policy on population growth and to prepare a proposal for a population council (Amani and Behnam, p. 65). At the same time the government invited a mission from the American Population Council in New York to advise on policy; in its report the mission favored emphasis on maternal health and family welfare, including the raising of living standards (Amani and Behnam, p. 65).
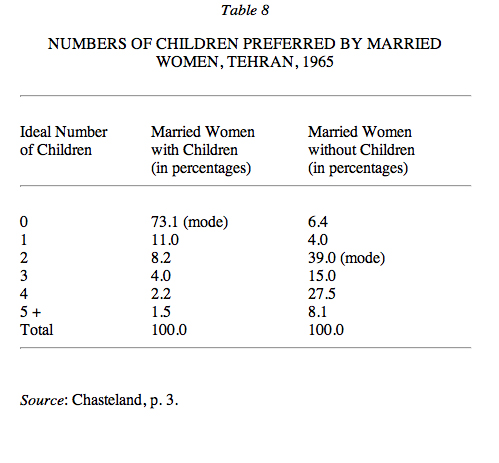
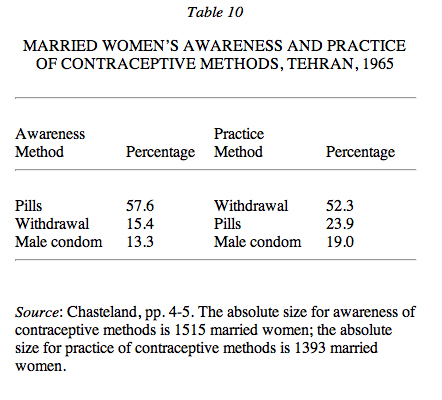
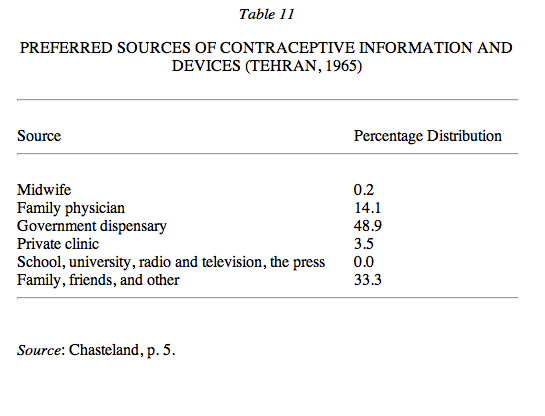
The 1965 demographic studies mentioned above had revealed potential acceptance of family planning among Persian women (Chasteland). Married women in Tehran were clearly open to birth control; although the average number of children born alive to this group was 5.8, the overwhelming majority of those studied considered the ideal number of children to be two to four (Table 7). Seventy-three percent of those with children expressed the desire to have no more (Table 8). Eighty-one percent of the women questioned were aware of the possibility of birth control, and nearly two-thirds favored it because of poverty or the need to care for children already born (Table 9). Although most of the women were aware of birth-control pills (Table 10), few were using them; the pills were still in a quasi-experimental stage in the 1960s, relatively expensive, and available only in cities. Of respondents using contraception 68 percent did so to prevent further births, 32 percent to control spacing of births. Preferred sources of birth-control information are shown in (Table 11). Nearly 67 percent preferred medical sources, and the more private network of family and friends was also of considerable importance. Some of the findings from this study helped to shape the official policy that was eventually adopted.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
THE FIRST PERIOD OF OFFICIAL FAMILY PLANNING
The Persian government feared that the combination of low mortality and high fertility was an obstacle to the nation’s socioeconomic development. The sometimes hesitant efforts outlined above thus culminated in the foundation, in 1967, of the Department of Health and Family Planning (Moʿāwanat-e behdāšt wa tanẓīm-e ḵānavāda) within the Ministry of Health; it was headed by Deputy Minister Amīr Manṣūr Sardārī.
The immediate task was enormous and difficult. The public had to be educated, demand for family-planning services had to be generated, and services adequate to meet this demand had to be developed. To implement these objectives, family-planning offices equipped with clinics and professional staff (doctors, midwives, nurses, social workers, etc.) were established in every important provincial city. By 1972 there were more than 1,500 such centers in operation (Dānešgāh, p. 35). The department remained active for a decade, through the period of the fourth (1968-1972) and fifth (1973-77) national economic plans.
{kind=link}
{kind=link}
The official preference was for oral contraceptives, rather than intrauterine devices, partly because some physicians and midwives had difficulty inserting the latter and women were reluctant to be examined by male physicians (Liberman, Gillespie, and Loghmani, p. 135). Nevertheless, if, in 1966-67, the government had planned to provide the pill to only 10 percent of the female population between the ages of fifteen and forty-four years (approximately 400,000 women), demand would have reached 5.2 million pills in that year alone (calculated on the basis of thirteen cycles a year for each woman). Given the annual population increase, the total demand, even among 10 percent of Persian women, would rise. For the government to distribute or sell the pill in 272 towns and tens of thousands of villages, where many could not afford to buy it, would thus have been an enormous undertaking. In fact, distribution of the pill through the private sector was far more effective. Although the price at the pharmacy in 1972 was approximately equivalent to 75 cents per cycle (compared to 13 cents at rural and 26 cents at urban dispensaries operated by the government), there were more pharmacies, which were easier to get to and often open twenty-four hours a day. Furthermore, pharmacies frequently sold the pill without prescription and more discreetly (Majalla-ye pezeškī-e nabzµ 2, 1370 Š./1991/, p. 4).
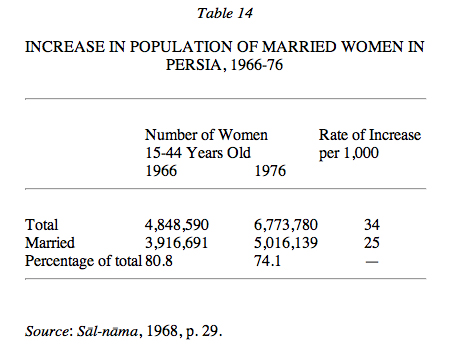
At the beginning of the official family-planning program the total number of women in Persia using contraceptives was 10,500, only 0.3 percent of the entire population of married women between the ages of fifteen and forty-four years. The population initially targeted consisted of married women between the ages of twenty and thirty-five years, nearly 60 percent of all married women of childbearing age ((Amani, 1970, p. 19; Table 14). This decline in the marriage rate was independent of family planning, but it was a positive factor in the success of that program.
{kind=link}
In 1970 the Department of Family Planning embarked upon an effort to reduce the rate of population growth in Persia to 1 percent by 1990, an annual reduction of 1 per 1,000 over a period of twenty years. Theoretically this goal was within the realm of possibity, particularly as underlying sociodemographic patterns seemed favorable. In fact, the projections were optimistic (Table 15), based on a presumed very rapid drop in the birth rate combined with a slow decline in mortality. In November 1972 the ministries of health and education sponsored a national seminar on education in demography, with the assistance of the World Health Organization (Geneva) and the Population Council, which already had an office of technical assistance in Tehran. It was a first step toward introducing the concept of population control into the Persian educational system, in order to engender responsible attitudes toward fertility and bring about the desired reduction. In 1973 abortion, considered an effective means of regulating births, was legalized under certain conditions. Another important factor was financial assistance from the United Nations Fund for Population Activities, which amounted to a cumulative total of $2.5 million by 1978.
{kind=link}
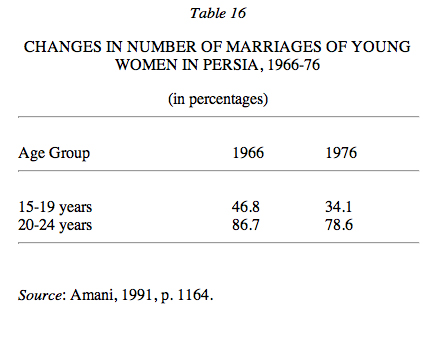
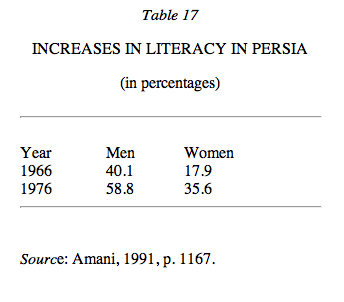
Overall, during the period 1966-76 various types of social change affected the family planning program positively, including a drop in the marriage rate among women aged fifteen to twenty-four years (Table 16); an increase in urbanization from 39 to 47 percent; and an increase in literacy (Table 17), which led married couples to assume a more responsible attitude toward procreation (Paydarfar and Sarram, p. 12). In turn the program produced a number of favorable demographic results, including a decline in the population below the age of fifteen years from 46.1 to 44.4 percent. The birth rate dropped sharply in the same period, an index of the program’s success.
{kind=link}
{kind=link}
THE POST-REVOLUTIONARY PERIOD
Since the revolution of 1357 Š./1978 family planning in Persia has passed through two distinct phases, first, the abolition of the existing government program (1979-88) and, second, the return to a vigorous campaign for family planning (mid-1988 to the present).
First phase. After the establishment of the Islamic Republic in February 1979 official family-planning programs were completely halted. One immediate result was a rise in the number of births to 1,691,000 in 1979, compared to an average of 1,355,000 in the five preceding years. According to official government data (Sāl-nāma, 1371, p. 49), the average annual number of births in the seven-year period 1980-86 was 2,200,000; there was a drop in 1987-88, probably owing to conditions arising from the war with Iraq.
During the war the “population factor” was considered by the government and by the Persian public as a strength. A study of fertility rates among females in the years 1976-86 revealed an approximate stability in the numbers of children borne by women between fifteen and twenty-nine years of age, whereas the average for women aged thirty to forty-four years was far higher in 1986 than in 1976. This group, of course, included mothers of sixteen- and seventeen-year-old boys, of whom many died in the war. The change in the birth rate (Āqājānīān, p. 31) suggests that grieving mothers were seeking to “replace” their dead sons.
Second phase. After the end of the war in 1988 high population growth, as revealed in the 1986 census (see Table 2), was recognized by the government as an obstacle to socioeconomic development. Control of demographic pressure on available resources seemed imperative, and, as a result, in June 1988 birth control was again authorized by ministerial decree, and the government initiated a family-planning program even more intensive than its predecessor. Every effort was made to impress upon officials and the public the urgency of the problem.
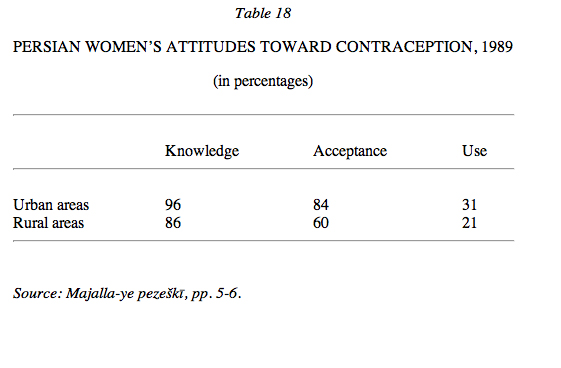
In September a large-scale seminar on population and development was sponsored by the Plan Organization, with the cooperation of relevant ministries and the universities. The objective was to study the issues from economic, social, medical, religious, and demographic points of view and to formulate a coherent population policy as part of the first five-year development plan (1989-93). The importance of sanitary conditions, especially for children, was stressed, in recognition that fear of losing children provokes behavior intended to minimize losses (see Grant, p. 8). The results of a study of married women in the childbearing years (Table 18) conducted in 1989 were taken as the basis for population policy, and the Ministry of health began vigorous propagation of family planning, left in abeyance for nearly a decade (Zanjānī, p. 171).
{kind=link}
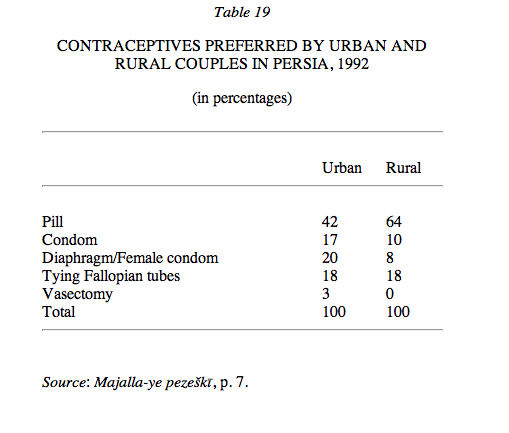
On 26 August 1990 the Council of Ministers delineated the family-planning responsibilities of the relevant minstries (Health, Education, Higher Education, Culture and Islamic Guidance, Labor and Social Affairs) and the Office of Vital Records (Jamʿīyat, nos. 5-6, 1372 Š./1993, pp. 86-87). In 1992 a similar study was conducted by the Department of Family Planning of the Ministry of Health to determine strategy during the second five-year plan (1994-98). It revealed that 47 percent of urban couples of childbearing age and 41 percent of comparable rural couples favored reliable and efficient birth control. The relative weight granted to these two characteristics differed between urban and rural areas, however (Table 19). The 1992 study also revealed the age structure among women contraceptive users (Majalla-ye pezeškī, p. 7).
{kind=link}
Optimum family size as defined at the 1988 seminar and integrated into the family-planning law of 16 May 1993 is three children; families with more are not eligible for additional family allowances from the government. The Ministry of Health plays the principal and immediate role in the control of fertility. In a report issued on World Population Day, 11 July 1992, the minister, Dr. ʿAlī-Reżā Marandī, declared birth control one of the important bases of general state policy. All contraceptives were to be provided free of charge. Four hundred hospitals were equipped to tie Fallopian tubes, and 200,000 women underwent the operation in 1991. More than 45 percent of married women between the ages of fifteen and forty-five years had already been reached by the family-planning program, and it was planned to increase the figure to 60 or 70 percent during the second five-year plan (Majalla-ye pezeškī, p. 6).
=
A number of factors recorded between the years 1986 and 1991 may lead directly or indirectly to some reduction in fertility. They include a rise in the average age of women at marriage from twenty to twenty-one years, a rise in the rate of urbanization from 54 to 57 percent, a rise in the literacy rate from 57 to 74 percent, and a drop in the proportion of married women in the childbearing years from 76 to 73 percent. Yet the generations of women who will reach their childbearing years in the near future have already been born. In the year 2001 there will be 16,260,000 women in this group; should the 1991 fertility rate (139 births per 1,000 women) continue, they will bear 2,260,000 babies a year, for an average overall increase in birth rate of 3.63 percent, much higher than the overall rate of population increase, which was about 1.8 percent for 1993, compared to 2.3 for 1992. Persia must thus aim at a birth increase rate lower than the population growth rate if the latter is to decrease.
Bibliography (for cited works not given in detail, see “Short References”):
M. Amānī, “Mawālīd wa bārvarī dar Īrān,” in Ānālīz-e saršomārī-e 1345 Īrān, Tehran, 1349 Š./1970.
Idem, “Situation démographique de l’Iran en 1991,” Revue Population 4-5, 1994, pp. 1159-69.
Idem and Dj. Behnam, La population de l’Iran, Paris, 1974.
A. Āqājānīān, “Taḥawwolāt-e jamʿīyatī-e Īrān dar ṣad sāl-e aḵīr,” Kelk 57, Āḏar 1373 Š./December 1994, pp. 27-35.
Bulletin d’information de l’Institut National d’Études Démographiques 171, 1983, pp. 1-4; 216, 1987, pp. 1-4; 259, 1991, pp. 1-4.
J. C. Chasteland, “Quelques données sur les attitudes à l’égard de la famille et de la régulation des naissances parmi les femmes mariées de Téhéran,” in 10ème Séminaire International de Recherche sur la Famille, 5 á 12 mars 1968, Tehran, 1968, pp. 1-7.
Idem et al., Étude sur la fécondité et quelques caractéristiques des femmes mariées dans 4 zones rurales d’Iran, Tehran, 1968.
Dānešgāh-e Tehrān, Dāneškada-ye behdāšt, Gozāreš-e nehāʾī-e semīnār-e āmārhā-ye behdāštī wa ḥayātī dar Īrān 14-17, Tehran, 1973.
A.-Q. Darbandī and Ḥ Ḵazāna, Pīšbīnī wa goḏaštanegarī-e jamʿīyat-e Īrān, Tehran, 1353 Š./1974.
J. Grant, “Mortalité infantile et croissance démographiqie” in Association: Equilibre & Population 8, February 1995, p. 8.
Jamʿīyat 5-6, 1972 Š./1993.
S. Liberman, R. Gillespie, and P. Loghmani, Projet d’information d’Ispahan IV, New York, 1973.
Ḥ. Malak-Afżalī, “Population and Family Planning in the Islamic Republic of Iran,” Majalla-ye pezeškī-e māḥāna-e nabż 2, 1371 Š./1992, pp. 2-7.
M.-Ḥ. Najātīān, Ofūl-e rošd-e šetābān-e jamʿīyat dar Īrān, Tehran, 1372 Š./1993.
A. Paydarfar and M. Sarram, “Differential Fertility and Socioeconomic Status of Shirazi Women,” International Journal of Marriage and Family 7/18, November 1970, pp. 131-41.
United Nations, World Population Prospect, Population Studies no. 86, New York, 1985.
Idem, Population Chart, ST/ESA Series A/116, New York, 1990.
J. Vallin, Population mondiale, Paris, 1989.
Ḥ. Zanjānī, Jamʿīyat wa šahrnešīnī dar Īrān, 2 vols., Tehran, 1370 Š./1991.
Attitudes affecting family planning in Afghanistan vary from condemnation to a growing awareness of the benefits of pregnancy spacing and limitation.
Family planning concepts first received official government sanction when the Family Guidance Association (Anjoman-e rāhnemā-ye ḵānavāda) was established on 22 July 1968 within the Ministry of Public Health under the patronage of Princess Maryam (L. Dupree, 1970a, p. 4). The term rāhnemāʾī (“guidance”) was intentionally selected so as to reinforce the voluntary aspect of the intended services and to avoid implication of government imposition.
In addition to dispensing pills and IUDs, the program consisted of training courses for family guidance medical and extension personnel, countrywide seminars for directors of provincial health institutions heads of basic health centers and midwives, the dissemination of information through films, and regular radio programs and a monthly journal. Association representatives attended international seminars in Tunisia, Cairo, London, and the United States.
The Afghan Family Guidance Association (FGA) was created as a private, national voluntary organization which was required to consult with the Ministry of Public Health only on matters of policy. Thus, the FGA received little monetary assistance from the Ministry. Major funds were provided by the International Planned Parenthood Foundation and bilateral international donors (L. Dupree, 1970b, p. 14).
In order to offset opposition from conservative Islamic leaders and to justify its services in communities where numbers of societal goals valued fertility and fostered negative attitudes toward the limitation of pregnancies (L. Dupree, 1970a, p.3), the government obtained a fatwā (q.v.) from al-Azhar University in Cairo, the major arbiter of religious interpretation in the Sunni Muslim world. The fatwā stated that, since the family is sacred to Islam and as children are important perpetuators of the family, Islam does not forbid married couples from practicing temporary birth control in order to ensure better health and education as well as to enhance the psychological and economic well-being of mothers and children. However, key stipulations forbade forced imposition of family planning by public law, insisted that planning methods be adopted as a matter of individual choice agreed to by both husband and wife, and declared unlawful the use of medicines and practices causing permanent control (L. Dupree, 1970a, p.10).
By 1977 the concept of voluntary family guidance had been gradually integrated into basic health services, and 37 FGA clinics were functioning in provincial towns and cities, with the majority concentrated in the capital city of Kabul (Ministry of Information, 1978, p. 664). In 1978 the countryside rose in revolt against the newly installed leftist government in Kabul and during the next 14 years of war over three million Afghans fled to refugee camps in Pakistan and Persia. Conservative attitudes, particularly against family planning, once again rose to the fore; reinforced by a natural desire of societies to repopulate in time of war, they caused fertility rates to reach world-record highs. By 1987 the high prewar marital fertility rate of 9.4 percent had risen to 13.6 percent (O’Connor, 1994, p. 166), and the age-specific fertility rate failed to show a normal rapid decline in women over 40 (Wulf, p. 42).
Health providers consequently intensified procedures for delivering their key message that high maternal and child mortality can be reduced when women learn to control their fertility. As a result, growing numbers of both men and women, among the refugees and at clinics inside Afghanistan, again seek guidance in family planning.
Bibliography
Afghan Family Guidance Association, First Annual Report, Kabul, 1969.
L. Dupree, Population Dynamics in Afghanistan, South Asia Series 14/7, 1970a, pp. 4-11.
Idem, Population Review 1970: Afghanistan, South Asia Series, 15/1, 1970b, pp. 13-15.
N. H. Dupree, The Present Role of Afghan Refugee Women and Children, The Hague, 1992, p. 6.
P. A. Hunte, “Indigenous Methods of Fertility Regulation in Afghanistan,” in L. F. Newman, ed., Women’s Medicine: Cross-Cultural Study of Indigenous Fertility Regulation, New Brunswick, 1985, pp. 43-75.
G. B. Kerr, Afghan Family Guidance Clients and Their Husbands Compared with Non-Client Neighbors and Their Husbands, Kabul, 1975.
G. B. Kerr et al., Indigenous Fertility Regulation Methods in Afghanistan, Kabul, 1975.
E. Krijgh, Health Status of Afghan Women and Children: An Assessment of Trends in 10 Refugee Camps between Hangu and Thal, Peshawar, 1987, pp. 4, 9, 28-33.
A. Macey et al., Indigenous Medical Practitioners in Afghanistan, Kabul, 1975.
Afghan Ministry of Information and Culture, The Kabul Times Annual 1970, Kabul, 1970, p. 387.
Idem, Afghanistan Republic Annual 1976, Kabul, 1976, p. 413.
Idem, Republic of Afghanistan Annual 1978, Kabul, 1978, pp. 663-65.
Ministry of Public Health, Infant and Early Childhood Mortality in Relation to Fertility Patterns, Kabul, 1978.
R. W. O’Connor, Managing Health Systems in Developing Areas: Experiences from Afghanistan, Lexington, Mass., 1980, pp. 163, 188-90.
Idem, Health Care in Muslim Asia: Development and Disorder in Wartime Afghanistan, Lanham (Maryland), 1994, pp. 166, 180-81.
State University of New York, National Demographic and Family Guidance Survey of the Settled Population of Afghanistan, 2 vols. Buffalo, 1975.
R. A. Stone and G. B. Kerr, Afghan Pharmacists: Their Knowledge and Attitudes Towards Family Guidance, Kabul, 1973.
M. de L. Verderese and L. M. Tumbull, The Traditional Birth Attendant in Maternal and Child Health and Family Planning: A Guide to Their Training and Utilization, Geneva, 1975.
D. Wulf, Refugee Women and Reproductive Health Care: Reassessing Priorities, New York, 1994, pp. 37-46.