
BEHDĀRĪ (maintaining health), term applied in Persian usage to the entire organization and services provided either by government or by various other agencies to secure the health of the people and consisting of hospitals, outpatient clinics, health centers, and other supporting services that function at different levels within the health care system and provide promotive, preventive, curative, and rehabilitative care.
Despite the advent of western physicians and the introduction of western medicine into Iran in the late seventeenth century and the foundation of the Polytechnic (Dār al-Fonūn) in the mid-nineteenth, at the outset of Reżā Shah’s reign (1299-1305 Š./1920-26) medicine in Iran was still predominantly Galenic in nature, based mostly on the traditional schools of Persian medicine of Avicenna and Abū Bakr Moḥammad Rāzī. Apart from limited preventive measures such as smallpox vaccination and quarantine services in southern and northern ports, health care during this period was primarily curative. The principal state health organizations were the State Health Council (Majles-e Ḥefẓ al-Ṣeḥḥat-e Dawlatī), which was established in 1283 Š./1904 as a central planning and governing body (Wezārat-e Eṭṭelāʿāt, p. 47) and health committees (hayʾat-e ṣeḥḥīya) administered by the Ministry of Education in five major cities and later by the Ministry of the Interior (Gilmour, pp. 31-54). The service infrastructure consisted of 21 hospitals (bīmārestān) with a total of 906 beds, which included 10 hospitals operated by foreign missionaries with a capacity of 650 beds; 90 urban dispensaries (darmāngāh-e šahrī); and 11 quarantine stations (īstgāh-e qaranṭīna) in the ports of the Persian Gulf and the Caspian Sea that were administered since 1849 by the East India Company in the south and by Russia in the north and, though put under Iranian authority on 17 Farvardīn 1306 Š./7 April 1927, continued to be staffed by non-Iranian institutions (Sotūda, p. 54). The total number of physicians, Iranian and foreign, was 945, including 293 graduates and 652 certified doctors (ṭabīb-e mojāz). Domestic medical education was confined to one college of medicine (madrasa-ye ṭebb), the offspring of the medical branch of the Polytechnic, which offered a five-year curriculum; a school of pharmacy (madrasa-ye dārū-sāzī) offering a three-year curriculum; and a school of midwifery (madrasa-ye qābelagī) also offering a three-year curriculum. Adjunct medical institutions were the Pasteur Institute (Moʾassasa-ye Pāstūr), founded in 1921 and charged with studying human and animal diseases, providing diagnostic services, and the preparing of vaccines and serums, and the Office of Schools of Health Administration (Edāra-ye Ṣeḥḥīya-ye Madāres) which was limited to Tehran and staffed by one physician. Certain groups within the population, such as the army, police, and employees of the Anglo-Iranian Oil Company, were also provided with their own organized health care. The organization charged with environmental hygiene, behdāšt-e moḥīṭ, existed primarily in name only. Vital and health statistics were rudimentary and unreliable and limited to Tehran. Health legislation during this period was limited to the Medical Practice Act of 1290 Š./1911 (Qānūn-e ṭebābat) and the Health Protection and Smallpox Vaccination Act of 1289 Š./1910 (Qānūn-e ḥefẓ al-ṣeḥḥa wa ābela-kūbī). Government health expenditures were very limited; the health budget for the fiscal year 1299 Š./1920 was estimated at 9 million rials (Sīmā-ye behdāšt wa darmān, p. 422).
The above organization and services could hardly cope with the health needs—much less the demands—of 10 million people (Gilmour, p. 14), nor could they protect the environment or prevent and control the major epidemics and endemics prevalent in Iran at the time. As a result plague (ṭāʿūn), cholera (wabā), small-pox (ābela), louse-borne typhus (moḥreqa), and influenza were common, and malaria (tab o nawba) was highly prevalent, causing 30-40 percent of all illness. More than 57 percent of the reported deaths in Tehran were caused by preventable infectious diseases almost half of which attacked children below the age of four.
Between the years 1304-58 Š./1925-79, health and medical care grew and developed extensively in Iran. In 1299 Š./1920, Dr. Moʾaddab-al-Dawla was appointed as Minister of Health and Welfare in the cabinet of Sayyed Żīāʾ-al-Dīn Ṭabāṭabāʾī and Dr. Ḥakīm-al-Dawla replaced him in 1300 Š./1921; but, after a period of inaction, the ministry was eliminated from the cabinet of Aḥmad Qawām (known as Qawām-al-Salṭana). The principal health care organization, the General Department of Health (Ṣeḥḥīya-ye Koll-e Kešvar) was established in 1305 Š./1926 under the Ministry of the Interior. The Ministry of Health (Wezārat-e Behdārī) was formed in 1320 Š./1941.
The Public Health Cooperative Organization (Sāzmān-e Hamkārī-e Behdāšt) was established in 1331 Š./1952 (Bāseqī, p. 221) in collaboration with the U.S. Point Four Program; its major concern was “promotive and preventive care” (erteqāʾ wa pīšgīrī-e behdāštī), i.e., those health needs that were mostly neglected by the Ministry of Health, because of the emphasis laid on curative care. The complete integration of the Public Health organization into the Ministry of Health did not come until 1341 Š./1962. Finally the Ministry of Health and Welfare (Wezārat-e Behdārī wa Behzīstī) was created in 1355 Š./1976.
The government began to see to the health insurance needs of workers late in the 1940s. In 1328 Š./1949, the Workers’ Social Insurance Organization (Sāzmān-e Bīma-ye Ejtemāʿī-e Kārgarān) was formed. Functioning first as a workers’ cooperative and insurance fund (ṣandūq-e taʿāwon wa bīma-ye kārgarān) under the Ministry of Labor and Social Insurance, the fund later, in 1333 Š./1954, expanded its coverage to include other groups. The Ministry of Health began to insure teachers and other government employees with the creation of an organization for the provision of curative services (Sāzmān-e Taʾmīn-e Ḵadamāt-e Darmānī) in 1342 š./1963. Medical and social insurance coverage was extended to farmers under the Ministry of Cooperatives and Rural Development (Wezārat-e Taʿāwon wa ʿOmrān-e Rūstāʾī) which was founded in 1348 Š./1969. Government health services were augmented by the Iranian Red Cross (Jamʿīyat-e Šīr o Ḵᵛoršīd-e Sorḵ-e Īrān) that was established in 1302 Š./1923 and which, since 1350 Š./1971, served as an important source of health care and health care workers. The Imperial Organization for Social Services (Sāzemān-e Šāhanšāhī-e Ḵadamāt-e Ejtemāʿī), established in 1326 Š./1947, helped provide health care in remote areas, prepare and distribute low-cost drugs, and train auxiliary health workers.
Privately funded health care organizations also brought medical services to rural Iran. In 1319 Š./1940 an organization for the protection of child-bearing women and neonates (Bongāh-e Ḥemāyat-e Mādarān o Nowzādān) was founded to provide maternity care in densely populated low-income class urban areas of Iran and to train auxiliary health care workers in mother and child care. The Shiraz Medical Center which was affiliated with the Iran Foundation (Bongāh-e Īrān) was created in 1335 Š./1956 to provide hospital care and to train health care providers. Eighteen medical schools with their extensive hospital networks were contributing to hospital and out-patient care, specialized care, and health manpower development.
In 1330 Š./1951 the health service department of the National Iranian Oil Company (Behdārī-e Šerkat-e Mellī-e Naft) with extensive health networks in all oil-producing areas was formed to replace the old Anglo-Iranian Oil Company health program. The army medical service (Behdārī-e Arteš) also maintained extensive health care facilities throughout the country, and, at the same time, other state-supported health care units were devoted to special groups within the population, e.g., the police, employees of the National Bank, and those working for the ministries of the roads, justice, economics, etc. Despite these advances, the development of health care in Iran was hampered by a lack of central planning and organization. Services provided by state and municipal organizations, on the one hand, and private groups, on the other, at times overlapped, causing wasteful duplication, while at the same time, because of maldistribution of services in terms of quantity and quality, segments of the population and some geographical areas could not be served properly.
With the rapid development and expansion of healthcare services in Iran, the Ministry of Health’s role as an organizer and coordinator of services became even more crucial. To handle its increasingly complex responsibilities the Ministry’s administrative structure expanded. The following five directorates were created, each headed by a vice-minister of health: 1. a vice-minister for parliament, legal affairs, information, and public relations; 2. a vice-minister for technical affairs to administer mass campaigns, including anti-malaria, public health and administration, curative-care services, food and drugs, diagnostic laboratories, nursing, medical social services, environmental health, and health education; 3. a vice-minister for planning and studies to administer units dealing with vital and health statistics, international health relations, technical education, budget, planning, and programming; 4. a vice minister for family health and family planning; 5. a vice-minister in charge of administration, personnel, security, transport, etc. In addition to this central apparatus, at a peripheral level, general departments of health (edāra-ye koll-e behdāšt) headed by director-generals, departments of health headed by county health commissioners, and district health centers headed by medical officers function in 23 provinces (ostān), 151 counties (šahrestān), and 459 districts (baḵš).
The Iranian health infrastructure was further elaborated with the creation of several national societies (jamʿīyat-e mellī) which served to alert the public about threats posed by specific diseases and to mobilize moral, material, and human resources in the effort to eradicate them (Sāzmān-e Šāhanšāhī-e Ḵadamāt-e Ejtemāʿī, pp. 119-32). In 1331 Š./1952 the National Society for the Protection of Children (Jamʿīyat-e Mellī-e Meḥāfaẓat az Kūdakān) was formed. This was followed by many societies, the most important of which were for aid to tuberculosis victims (komak be maslūlīn) in 1334 Š./1955, for the fight against cancer (mobāraza bā saraṭān) in 1335 Š./1956, for aid to lepers (komak be joḏāmīān) in 1339 Š./1960, for the control of zoonoses (mobāraza bā bīmārīhā-ye moštarak bā dām) in 1340 Š./1961, for aid to burn victims (komak be qorbānīān-e sūḵtagī) in 1345 Š./1966, and for aid to the blind and deaf (komak ba nābīnāyān wa karhā). In addition to these, a national blood transfusion organization (Sāzmān-e Mellī-e Enteqāl-e Ḵūn) was founded in 1351 Š./1972.
Medical education. From its modest beginnings in 1266/1850 with the foundation of the College of Medicine in the Tehran Polytechnic, Iranian medical education has grown significantly, especially since World War II. By 1300/1893, apart from the medical and pharmacological colleges of the Polytechnic and an American missionary school of nursing established in Reżāʾīya (Urmia) in 1294 Š./1915, there were no domestic institutions for the training of medical personnel; most students were obliged to pursue their medical education abroad. However, the situation changed markedly with the expansion of institutions of higher learning throughout Iran. By 1357 Š./1978 there were 18 medical colleges (dāneškada-ye pezeškī), 7 post-graduate training centers in various medical specialties (markaz-e āmūzeš-e taḵaṣṣoṣ-e rešta-ye pezeškī), a school of public health (dāneškada-ye behdāšt), departments of public health or community medicine in two medical colleges with post-graduate courses in public health, 32 nursing schools (āmūzešgāh-e parastārī), 90 schools for training assistant nurses (āmūzešgāh-e behyārī), 11 schools of midwifery and assistant midwifery (āmūzešgāh-e māmāʾī wa komak-māmāʾī), 60 schools for the training of health technologists and technicians, 5 centers for the training of rural health workers (markaz-e tarbīat-e kārkonān-e behdāštī-e rūstāʾī), 5 schools of pharmacy (dāneškada-ye dārū-sāzī), 5 schools of dentistry (dāneškada-ye dandān-pezeškī), 4 schools of veterinary medicine (dāneškada-ye dām-pezeškī), and 8 centers for training of technicians in pharmacy, dentistry, and veterinary medicine. The training of assistant physicians (behdār), established in 1319 Š./1940 in 3 centers but closed in 1332 Š./1953, was reinstated in 2 centers in 1354 Š./1975.
Allied with the regular medical colleges and health training centers were several institutes that conducted medical research and provided technical support to the health care effort. In addition to the Pasteur Institute, which was functioning since 1300 Š./1921, the Rāzī Institute of Veterinary Sciences (Moʾassasa-ye Vāksan wa Serom-sāzī-e Rāzī) was set up in 1310 Š./1931 to study animal diseases and prepare biological materials. An institute for public health research (Moʾassasa-ye Taḥqīqāt-e Behdāštī) was founded in 1331 Š./1952 to study the geographical pathology of Iran, epidemiology, and control of endemic diseases, and to conduct field trials of different control measures, health and manpower surveys, and health services research. In order to carry out research and diagnostic services in cancer, a cancer institute (Moʾassasa-ye Saraṭān) was created in 1335 Š./1956. In 1340 Š./1961, a food and nutrition institute (Moʾassasa-ye Taḡḏīa wa Ṣanāyeʿ-e Ḡeḏāʾī) was established to study the value of different local foods and to conduct research on nutritional diseases and deficiencies in Iran. Medical research in Iran was further enhanced with the establishment of the Fīrūzgar Medical Center in 1342 Š./1963, which performed clinical research and trials on various preparations. To report on medical advances within the country, several medical journals, some achieving international reputation and circulation were begun; in 1356 Š./1977, there were 21 such journals.
By the early 1970s, the Iranian health sector had proliferated to such a degree that the need for greater organization and coordination once again became acute. Thus one of the basic objectives of the fifth health development plan (Barnāma-ye behdāštī dar panjomīn barnāma-ye ʿomrānī-e kešvar) was the introduction of the health care system concept, according to which all units providing health care would be in some manner brought within a single network of comprehensive and coordinated services. To implement this concept, a three-tier design, i.e., a provision of health-care on three levels, within the pyramid of health-care, all coordinated and interconnected through “referral,” was introduced that consisted of: 1. primary medical care provided by local, “front line” health workers (behvarz, behdāštyār); 2. an intermediate service in county health centers in moderately-sized general hospitals; and 3. a tertiary care provided in specialized centers at provincial and municipal hospitals. Ancillary programs, i.e., mass campaign against diseases such as malaria, smallpox, tuberculosis, and leprosy were also introduced on a country-wide basis. These programs have proved quite effective: Smallpox has been eradicated; malaria, tuberculosis, preventable diseases of infancy (diphtheria, pertussis, measles, tetanus, poliomyelitis, etc.) have been well under control. To insure that the disadvantaged received their share of health services, a social security system (bīma-ye ejtemāʿī) having its own health insurance component was created in 1354 Š./1975.
During the 1960s, measures had been taken to decentralize the health care system so that rural people could obtain sophisticated treatment without having to travel to the cities. In 1343 Š./1964, the Health Corps (Sepāh-e Behdāšt), consisting of young volunteers who went to rural areas to work on rudimentary health and sanitation projects as part of their military service, was formed, and mobile and semi-mobile medical units were sent throughout the country under the auspices of the Ministry of Health (General Department of Health Corps) and the Iranian armed forces.
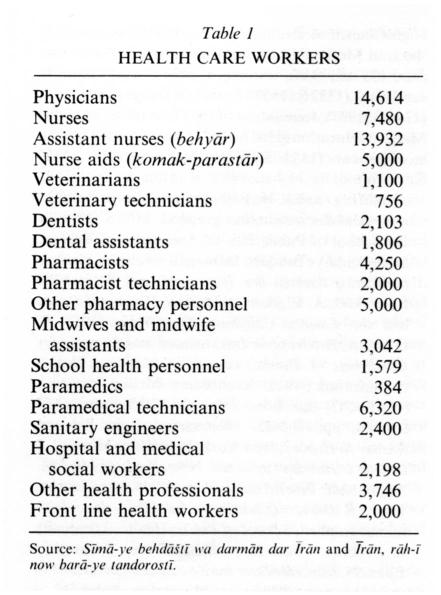
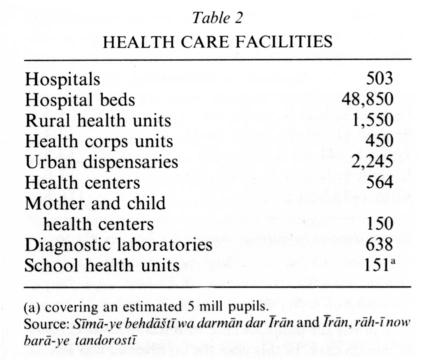
The number of health care workers and facilities (estimated 79,710) in mid-1357 Š./1978 are set out in Table 1 and Table 2.
{kind=link}
{kind=link}
In addition to these units, there were two leprosariums (joḏām-ḵāna), one leprosy rehabilitation village, and several “health houses” (ḵāna-ye behdāšt) located in several provinces.
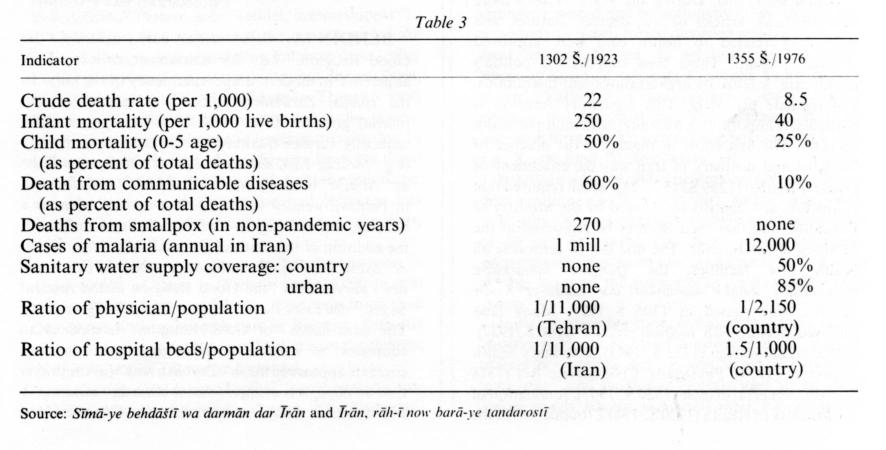
The impact of these human and material resources on the health of the people during the period 1302-57 Š./1923-78 has been great as shown by the major health indicators (taken at Tehran) set out in Table 3.
{kind=link}
In 1302 Š./1923 immunization against communicable diseases was limited to smallpox (no coverage), for 1355 Š./1976 the coverage shows an annual total of 5 million children.
Health expenditure. The first recorded annual expenditure for Iran, compiled in 1299 Š./1920, shows a total of Rls 228 million/5.4 million sterling pounds, with Rls 900,000/22,500 sterling pounds for health-care. In this year the oil revenue was Rls 32 million/800,000 sterling pounds. From then until 1327 Š./1948, allocation of funds for all programs, including health, was not based on sound planning and priorities were given mostly to biased demands rather than real needs. From 1948 allocation of funds for health-care were made on a seven/five-year basis and the instrument for proper planning and programming, a joint planning committee of the Ministry of Health and Plan Organization, was established. During the period 1327-53 Š./1948-74, the amounts spent on health-care increased from Rls 1.5 to 116.5 billion/$22-166 million (see Table 4) and, for the single year of 1974, the total government and health expenditures and the oil revenue were respectively 1089, 35, and 445 billion/$15.5, 0.5, and 6.5 billion. These figures show a 47.700-, 38.800-, and 14.000-fold increase respectively over those of 1920. The consumer index for the same period had increased 45 times, so the corrected increase was 1060, 864, and 311 times. However, while this increase in the health-care expenditures is encouraging, still the health sector does not receive the expected percentage of the total government budget (actual 3.2-3.5 percent against expected 6.5 percent).
{kind=link}
Health legislation. During the years 1926-76 more than 160 laws, articles of law, decrees, statutes, and regulations related to health care were approved (Sotūda, passim). These laws support the nation’s health care, legalize its organizations and institutions, and regulate providers. This regulatory function is particularly important in a country with multiple health agencies. The first effort to regularize the practice of medicine and dentistry in Iran was the enactment or Qānūn-e ṭebābat (1299 Š./1920-21), which required that all doctors and dentists be licensed by the Ministry of Education and that their licenses be registered at the Ministry of the Interior. The first law to centralize all health care facilities, the Qānūn-e tamarkoz-e moʾassasāt-e ṣeḥḥī-e mamlakatī dar Edāra-ye Koll-e Ṣeḥḥīya, was passed in 1305 Š./1927. Many laws followed, dealing with: medical practice (1306 Š./1927), public immunization (1322 Š./1943), veterinary health inspection (1934), Physicians’ Civil Service Act (1318 Š./1939), venereal disease (1320 Š./1941), foundation of the Ministry of Health (1320 Š./1941), foundation of the High Council of Health (1329 Š./1950), foundation of the Iran Medical Council (Qānūn-e neẓām-e pezeškī-e Īrān, 1337 Š./1958), training of physicians to serve in rural areas (1337 Š./1959), Food and Drugs Control Act (1346 Š./1967), foundation of the National Council for Medical Education (1352 Š./1973), protection of human environment (1353 Š./1974), social security (1354 Š./1975).
Bibliography:
Ḥ. Bāseqī, Sāzmānhā-ye behdāštī o darmānī dar Īrān, mimeographed, 1353 Š./1974, at the School of Public Health, University of Tehran. Dāneškada-ye Behdāšt, Dānešgāh-e Tehrān, Sīmā-ye behdāštī o darmān dar Īrān, publ. no. 2013, 1353 Š./1974.
C. A. Elgood, A Medical History of Persia and the Eastern Caliphate, Cambridge, 1951.
J. Gilmour, Report of an Investigation into the Sanitary Conditions of Persia, League of Nations, Health Organization, 1925.
Komīsīūn-e Mellī-e Yūnesko (UNESCO) dar Īrān, Īrān-šahr II, Tehran, 1343 Š./1964, pp. 1402-52.
Moḥammad Reżā Pahlavi, Answer to History, New York, 1980.
R. S. Morton, A Doctor’s Holiday in Iran, New York, 1940.
M. Najmābādī, Pezeškī dar Īrān baʿd az Eslām, Tehran, 1353 Š./1974.
Qawānīn-e behdāštī dar Īrān, mimeographed, School of Public Health, University of Tehran. Sāzmān-e Šāhanšāhī-e Ḵadamāt-e Ejtemāʿī, Īrān, rāh-ī now barā-ye tandorostī, report of the Hayʾat-e Barrasī-e Masāyel-e Behdāštī o darmānī-e Kešvar I, 1353 Š./1974, II, 1354 Š./1975.
N. Sotūda, “Tārīḵ-e Behdārī,” in Tārīḵ-emoʾassasāt-e ʿelmī o āmūzešī-e Īrān, mimeographed, 1350 Š./1971.
Idem, “Naqš-e dawlat dar behdāšt o darmān,” in A. A. ʿĀlemī, ed., Oṣūl o janbahā-ye modīrīyat-e behdāšt-e ʿomūmī, Tehran, 1357 Š./1978, pp. 320-33.
Wezārat-e Behdārī, Īrān, 1348 Š./1969.
Wezārat-e Eṭṭelāʿāt, Īrān, 1348 Š./1969.
WHO Health Service Development Research, unpubl. interim document, 1973, School of Public Health, University of Tehran.
Search terms:
| بهداری | behdari | behdaari | behdary |
(Mohammad Ali Faghih)
Originally Published: December 15, 1989
Last Updated: December 15, 1989
This article is available in print.
Vol. IV, Fasc. 1, pp. 100-104
Mohammad Ali Faghih, “BEHDĀRĪ,” Encyclopaedia Iranica, IV/1, pp. 100-104, available online at http://www.iranicaonline.org/articles/behdari (accessed on 30 December 2012).